Clinical evidence
inspIRE
The VARIPULSE™ Platform first-in-human study
Key results included the following: 0% primary adverse events and 80% 12-month effectiveness with optimal PFA applications.1,2
Study Design
About this study
The inspIRE study evaluated the safety and effectiveness of the VARIPULSE™ Platform (VARIPULSE™ Catheter and TRUPULSE™ Generator) with CARTO™ 3 System integration for the treatment of drug-refractory paroxysmal atrial fibrillation in European and Canadian populations.
Design
This was a prospective, multicenter, nonrandomized study that included 226 participants with drug-refractory symptomatic PAF at 13 European and Canadian centers.
Endpoints
Primary Safetya
Primary adverse events: Predefined primary adverse events within 7 days postablation
Primary Effectivenessb
Freedom from documented atrial tachyarrhythmia during the evaluation period and freedom from acute failure
Patient eligibility criteria
266 participants with symptomatic paroxysmal AF were enrolled in the study in 13 centers in Europe and Canada.
- 18–75 years old
- Diagnosed with symptomatic paroxysmal AF
- Selected for AF ablation procedure by PVI
- Failed/intolerance to ≥1 Class I–IV AADs
- AF secondary to reversible or noncardiac cause
- Previous surgical or catheter ablation for AF
- Anticipation of receiving ablation other than PVI
- Persistent AF
Follow-up
Months 1, 3, 6, and 12
Stringent Monitoring
- Remote arrhythmia monitoring: Weekly between months 3–5, monthly between months 6–12, when symptomatic
- 24-hour Holter: months 3, 6, 12
- ECG: Standard of carec
Wave I
n=40, Safety characterization
Wave II
n=186, Safety and effectiveness up to 12 months

Follow-up
Months 1, 3, 6, and 12
Stringent Monitoring
- Remote arrhythmia monitoring: Weekly between months 3–5, monthly between months 6–12, when symptomatic
- 24-hour Holter: months 3, 6, 12
- ECG: Standard of carec
Wave I
n=40, Safety characterization
Wave II
n=186, Safety and effectiveness up to 12 months
Results
Safety

0%
primary adverse event rate

0%
esophageal lesions of thermal origin, PV stenosis, or coronary spasm in Wave I
Sedation compatibility
Approximately 30% of procedures among Wave II participants were performed under conscious sedation. The use of general anesthesia or sedation did not affect the primary effectiveness outcome (OR 0.46; 95% CI 0.23 to 0.93, P<0.20).2
A single-center analysis of 29 cases ablated with a deep sedation protocol demonstrated a good safety profile with positive participant-reported satisfaction.4
Effectiveness
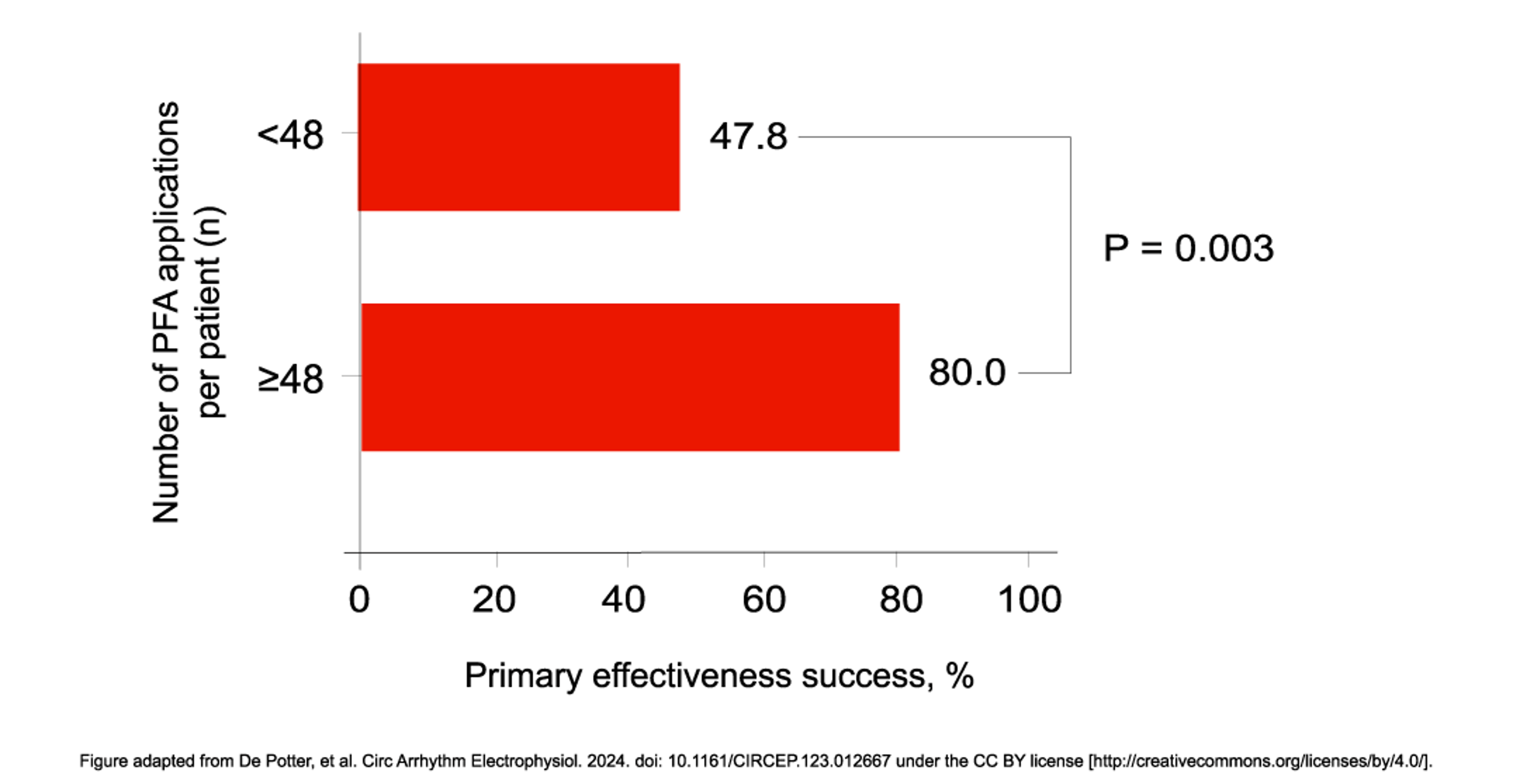
A primary effectiveness of 80% was achieved in participants receiving optimal PFA applicationsd of 48 or more (n=158)
The primary effectiveness endpoint was 75.6% (95% CI 69.5% to 81.8%) for the full per-protocol cohort; therefore, the primary effectiveness endpoint was met (50% performance goal). Twelve-month freedom from repeat ablation postblanking was 92.4% (2-sided 95% CI 88.5% to 96.2%).
Figure adapted from De Potter, et al. Circ Arrhythm Electrophysiol. 2024. doi: 10.1161/CIRCEP.123.012667 under the CC BY license.
Fluoroscopy exposure
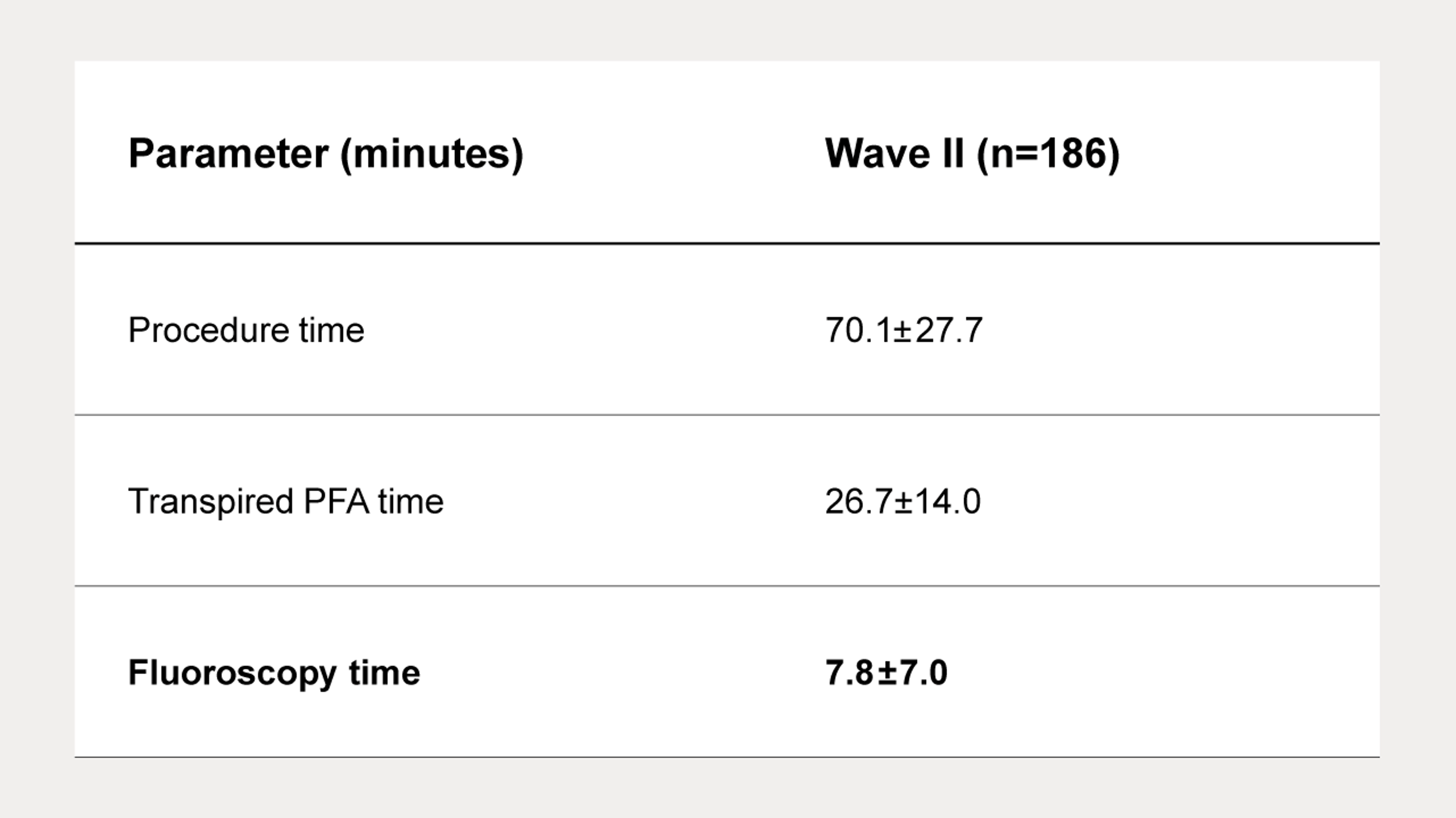
CARTO™ 3 System integration minimizes fluoroscopy exposure1
Mapping system integration allowed operators to place the catheter by identifying and eliminating electrode overlaps, while ensuring that energy application was delivered around the entire vein without gaps. The short fluoroscopy time is at par with that observed for the latest radiofrequency ablation technology.3
Conclusions
The inspIRE study met its safety and effectiveness endpoints.
- No primary adverse events were reported in the study, and the 12-month effectiveness was 80% with optimal PFA applications.
- The VARIPULSE™ Platform integrated to the CARTO™ 3 System supported a low fluoroscopy workflow.

The inspIRE study met its safety and effectiveness endpoints.
- No primary adverse events were reported in the study, and the 12-month effectiveness was 80% with optimal PFA applications.
- The VARIPULSE™ Platform integrated to the CARTO™ 3 System supported a low fluoroscopy workflow.
References
Footnotes:
a. Primary adverse events were defined as myocardial infarction, thromboembolism, transient ischemic attack, diaphragmatic paralysis, pneumothorax, heart block, pulmonary edema, vagal nerve injury, pericarditis, major vascular access complication or bleeding, death, stroke, or any other cerebrovascular accident. Atrioesophageal fistula and PV stenosis occurring >7 days postablation along with cardiac tamponade or perforations occurring within 30 days of the ablation procedure were also considered primary adverse events.
b. Primary effectiveness was defined as 12-month freedom from documented atrial arrhythmia recurrence (AF/AT/AFL) post 3-month blanking period and freedom from acute failure.
c. ECG was conducted per each site’s standard-of-care practice; it was not mandated by the protocol to be completed on every visit.
d. Optimal PFA applications refers to 2 sets of ostial and 2 sets of antral PFA applications per PV; per subject, a total of 48 applications.
Abbreviations:
AAD, antiarrhythmic drug; AF, atrial fibrillation; AFL, atrial flutter; AT, atrial tachycardia; CI, confidence interval; ECG, electrocardiogram; LA , left atrium; OR, odds ratio; PFA, pulsed-field ablation; PV, pulmonary vein; PVI, pulmonary vein isolation.
References:
- Duytschaever M, De Potter T, Grimaldi M, et al. Paroxysmal AF ablation using a novel variable-loop biphasic pulsed field ablation catheter integrated with a 3D mapping system: 1-year outcomes of the multicenter inspIRE study. Circ Arrhythm Electrophysiol. 2023;16(3):e01178.
- De Potter T, Grimaldi M, Duytschaever M, et al. Predictors of success for pulmonary vein isolation with pulsed field ablation using a variable loop catheter with 3D mapping integration: complete 12-month outcomes from inspIRE. Circ Arrhythm Electrophysiol. 2024;17(5):e012667.
- Osorio J, Hussein AA, Delaughter MC, et al. Very high-power short-duration, temperature-controlled radiofrequency ablation in paroxysmal atrial fibrillation: the prospective multicenter Q-FFICIENCY trial. JACC Clin Electrophysiol. 2023;9(4):468-480.
- Grimaldi M, Auandrini F, Caporusso N, et al. Deep sedation protocol during atrial fibrillation ablation using a novel variable-loop biphasic pulsed field ablation catheter. Europace. 2023;25(9):euad222.
VARIPULSE™ Platform preclinical studies:
- Yavin H, Brem E, Zilberman I, et al. Circular multielectrode pulsed field ablation catheter lasso pulsed field ablation: lesion characteristics, durability, and effect on neighboring structures. Circ Arrhythm Electrophysiol. 2021;14(2):e009229.
- Hsu JC, Gibson D, Banker R, et al. In vivo porcine characterization of atrial lesion safety and efficacy utilizing a circular pulsed-field ablation catheter including assessment of collateral damage to adjacent tissue in supratherapeutic ablation applications. J Cardiovasc Electrophysiol. 2022;33(7):1480-1488.
- Grimaldi M, Di Monaco A, Gomez T, et al. Time course of irreversible electroporation lesion development through short- and long-term follow-up in pulsed-field ablation–treated hearts. Circ Arrhythm Electrophysiol. 2022;15(7):e010661.
- Hsu JC, Banker RS, Gibson DN, et al. Comprehensive dose–response study of pulsed field ablation using a circular catheter compared with radiofrequency ablation for pulmonary vein isolation: a preclinical study. Heart Rhythm O2. 2023;4(10):662-667.
Disclosures:
Important information: Prior to use, refer to the instructions for use supplied with the device for indications, contraindications, side effects, warnings and precautions. The VARIPULSE™ Catheter and the TRUPULSE™ Generator have received FDA approval in the United States, and CE mark for use in the European Union. For complete approved indications, please refer to the corresponding “Instruction For Use” online at e-ifu.com.
The THERMOCOOL SMARTTOUCH™ SF Catheter is indicated for the treatment of drug refractory recurrent symptomatic paroxysmal atrial fibrillation (AF) and for drug refractory recurrent symptomatic persistent AF (continuous AF > 7 days but < 1 year), refractory or intolerant to at least 1 Class I or III AAD, when used with the CARTO™ 3 System.
Always verify catheter tip location using common clinical practice for real-time verification (inspection of IC signals, direct imaging guidance such as fluoroscopy or ultrasound, etc.) and consult the CARTO™ 3 System User Guide regarding recommendations for fluoroscopy use.
Canpolat, U. et al (2020). State of Fluoroless Procedures in Cardiac Electrophysiology Practice. J Innov Cardiac Rhythm Management. 11(3), 4018–4029. Sommer, P. et al (2018) Safety profile of near-zero fluoroscopy atrial fibrillation ablation with non-fluoroscopic catheter visualization: experience from 1000 consecutive procedures, EP Europace, Volume 20, Issue 12, Pages 1952–1958.
This site is published by Johnson & Johnson and its affiliates, which is solely responsible for its contents. It is intended for visitors from the United States. Last Updated on 10/14/2025.
C_US_ELP_THER_303439.3.EN