smartfIRE
The Dual Energy THERMOCOOL SMARTTOUCH™ SF Platform European Study.
Key results included the following: 86.9%* 12-month effectiveness with high workflow adherence and acceptable safety1,2
Study Design
About this study
The SmartfIRE study evaluated the safety and effectiveness of the Dual Energy THERMOCOOL SMARTTOUCH™ SF Catheter with TRUPULSE™ Generator and CARTO™ 3 System integration for the treatment of paroxysmal atrial fibrillation.
Design
This was a prospective, multicenter, nonrandomized study that included 149 participants with drug-refractory symptomatic PAF at 9 European centers.1,2
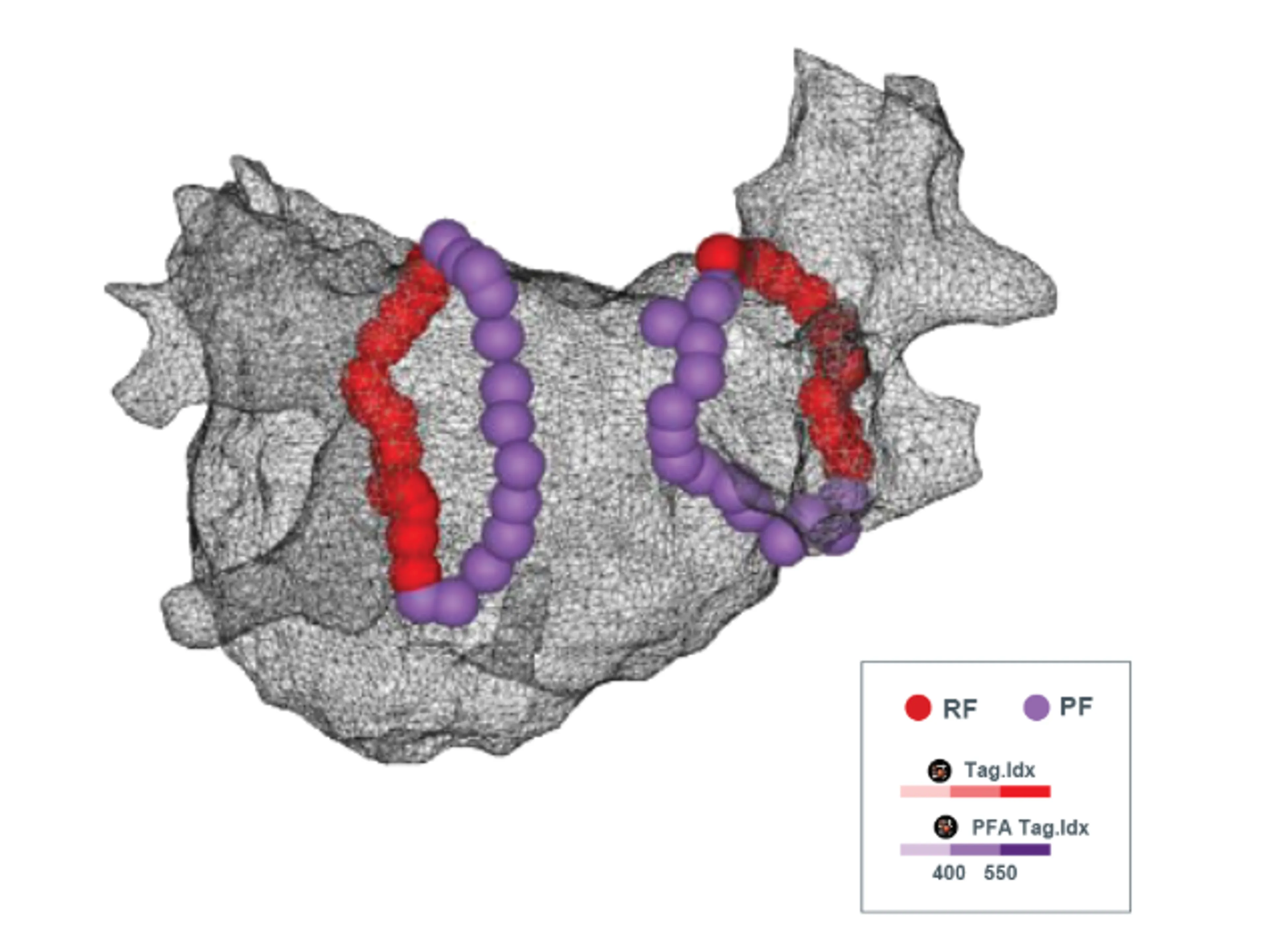
Recommended workflow
- PFA at posterior/inferior and RF ablation at anterior/ridge/carina segments
- Target index of 400 for posterior/inferior and 550 for anterior/roof/ridge/carina
- Tag size of 3 mm
- Inter-tag distance ≤6 mm
Patient eligibility criteria
- 18–75 years old
- Diagnosed with symptomatic paroxysmal AF
- Selected for catheter ablation procedure by PVI
- Failed/intolerance to ≥1 AADs (Class I–IV)
- Willing and capable of providing consent and comply with study testing and requirements
- AF secondary to reversible or noncardiac cause
- Previous LA ablation or surgery
- Anticipation of receiving ablation outside the PV region and outside the CTI region
- Previously diagnosed with persistent AF
- Life expectancy less than 12 months
Follow-up
Stringent Monitoring
- Remote arrhythmia monitoring: weekly between months 1–5, monthly between months 6–12, and when symptomatic
- 24-hour Holter: months 3, 6, 12
- 12-lead ECG: predischarge, and at months 1, 3, 6, 12

Follow-up
Stringent Monitoring
- Remote arrhythmia monitoring: weekly between months 1–5, monthly between months 6–12, and when symptomatic
- 24-hour Holter: months 3, 6, 12
- 12-lead ECG: predischarge, and at months 1, 3, 6, 12
Results
Effectiveness

12-month effectiveness2
- 71.5% freedom from documented AF/AFL/AT recurrencea
- 84.2% when using standard-of-care monitoringb
- 86.9% 12-month freedom from AF/AFL/AT recurrence in patients with high ablation workflow adherence (n=47)c
- 64.0% in patient with low workflow adherence (n=88)

Acute effectiveness1
- The primary effectiveness endpoint was met.d
- 100% Primary Effectiveness Endpoint
- 96.8% first-pass isolation (no acute reconnection) per vein
Safety1

4.4%
primary adverse event ratee,1

0%
coronary spasm, esophageal injury, phrenic nerve injury, hemolysis, or acute kidney injury.1,2
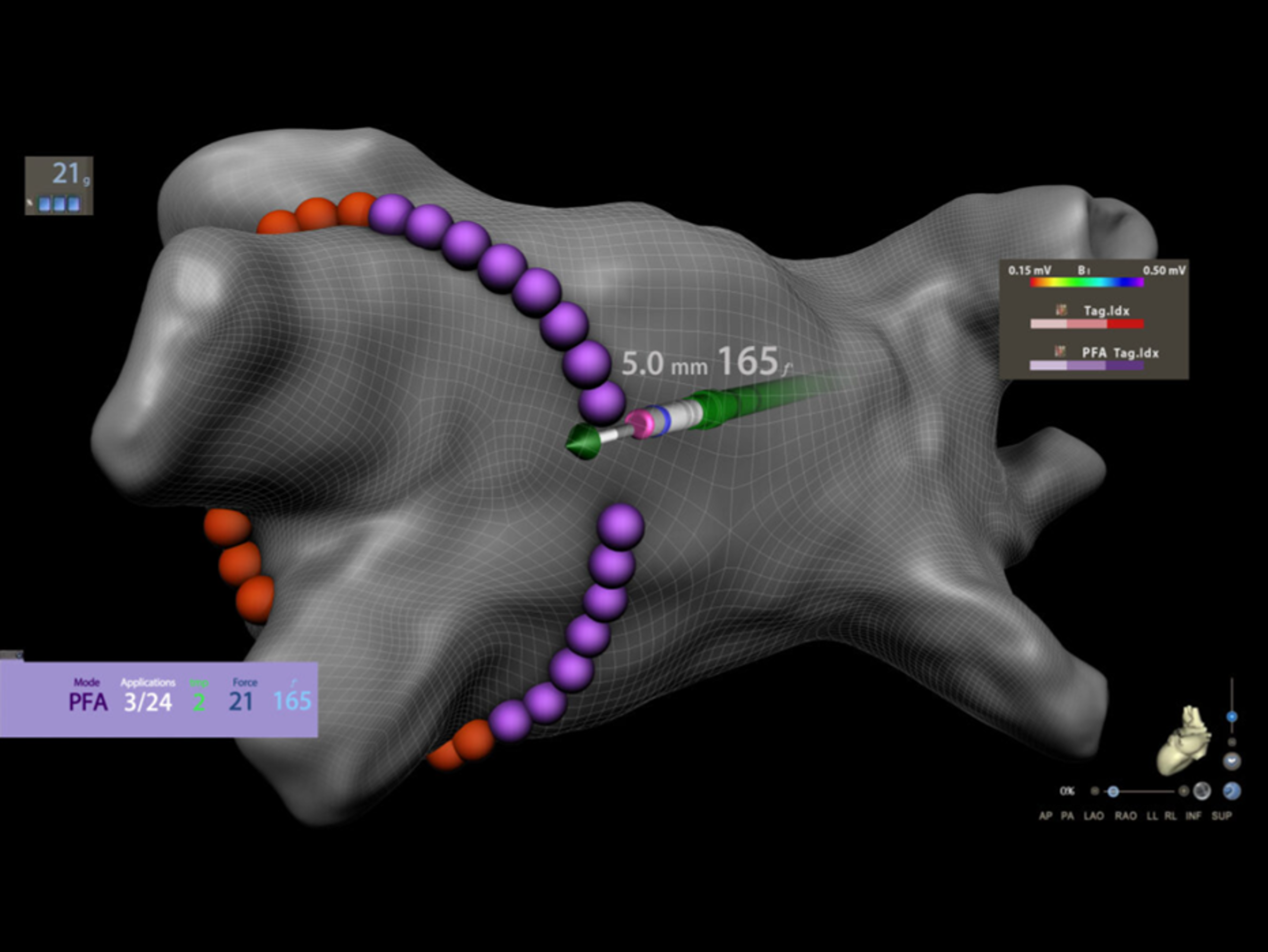
Procedural efficiency

CARTO™ 3 System integration increases procedural efficiency1
Mapping system integration allows real-time visualization of the catheter, increases procedural efficiency, and minimizes fluoroscopy exposure.
PVI durability1
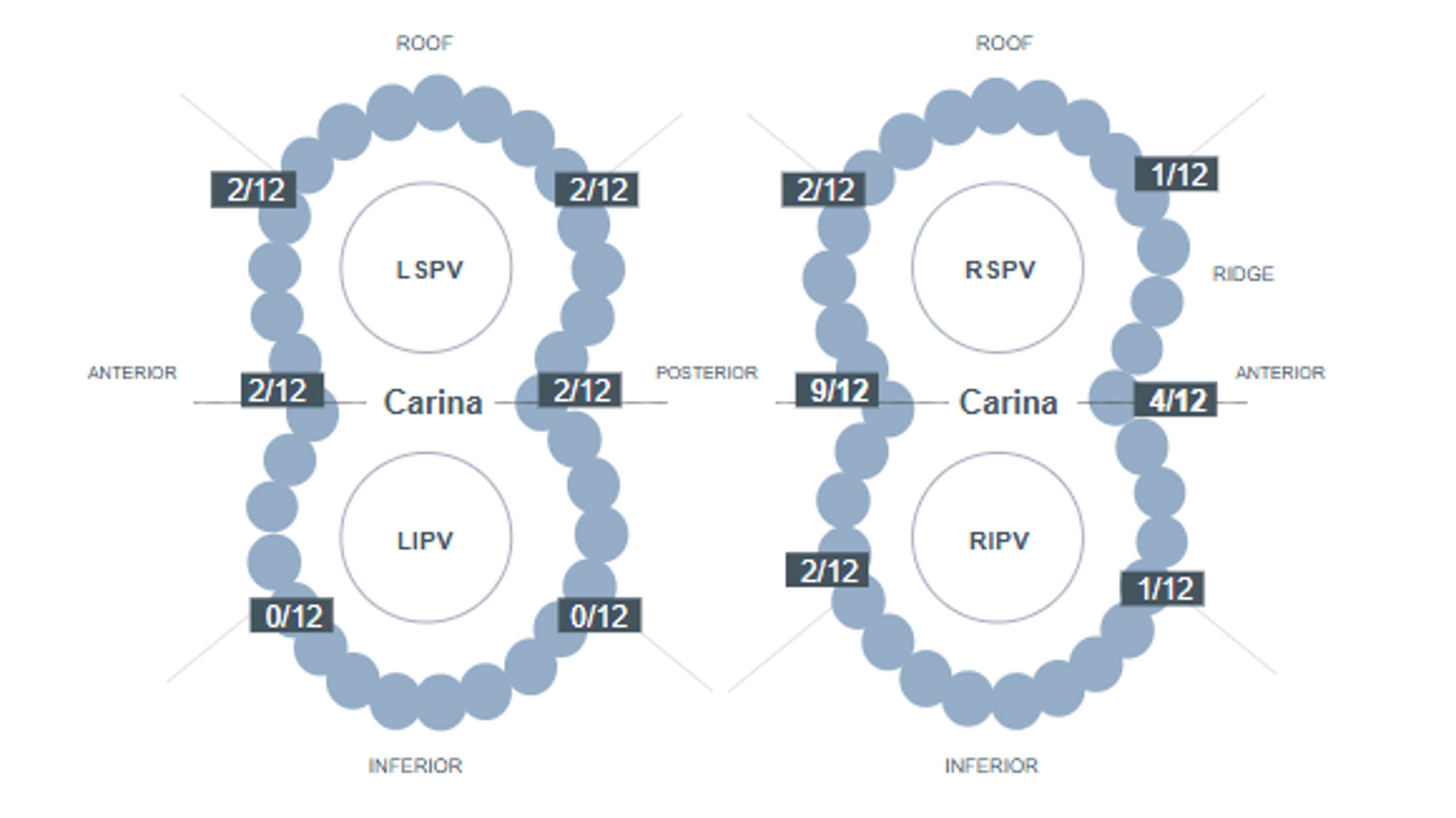
87% PVI durability (100/115 PVs) was observed1
- Prespecified subset of 30 patients underwent 3D electroanatomic remapping at a mean 79.3 ± 6.9 days postindex procedure regardless of symptoms
- Reconnections observed were due to noncontiguity (greater ITD) and lack of transmurality (lower ablation index and lack of stability) in the index procedure. A limitation is that in the study software version, system integrated catheter stability indicator was not available, and PF tags were applied without respiratory gating
Quality of life and healthcare utilization2
Compared to baseline, patients experienced significantly improved quality of life and reduced healthcare utilization 12 months (n=136)h.

Conclusions
The smartfIRE study met its safety and effectiveness endpoints.
- 71.5% 12-month effectiveness in the entire cohort and 86.9%* with high workflow adherence; 100% acute procedure success.
- The study reported an acceptable safety profile.
- The DE STSF Platform integrated to the CARTO™ 3 System supported a low fluoroscopy workflow.
- Patients experienced improved quality-of-life and reduced healthcare utilization.
The smartfIRE study met its safety and effectiveness endpoints.
- 71.5% 12-month effectiveness in the entire cohort and 86.9%* with high workflow adherence; 100% acute procedure success.
- The study reported an acceptable safety profile.
- The DE STSF Platform integrated to the CARTO™ 3 System supported a low fluoroscopy workflow.
- Patients experienced improved quality-of-life and reduced healthcare utilization.
References
Footnotes:
*86.9% is based on a post hoc subgroup analysis treated with adherence to the recommended ablation workflow.
a. Freedom from recurrence was defined as freedom from documented symptomatic and asymptomatic atrial arrhythmia (AF/AFL/AT) episodes based on electrocardiographic data (≥30 seconds on arrhythmia monitoring device) during the effectiveness evaluation period (Day 91–365) on or off antiarrhythmic therapy. Acute procedural failure was also considered a failure for this endpoint.
b. Standard-of-care monitoring included 12-lead ECG and 24-hour Holter but did not include TTM.
c. In a post-hoc analysis, the high adherence group consisted of patients with more than 95% of applications maintaining an ITD of ≤6 mm and over 70% of applications achieving a minimum PF/RF index of 400 in the posterior wall and 500 in the anterior wall of the PV regions. Patients not meeting these criteria were categorized into the low adherence group.
d. Primary effectiveness endpoint was acute procedural success, defined as electrical isolation of targeted PVs (confirmed by final entrance block) after adenosine/isoproterenol challenge at the end of the index ablation procedure. Use of a nonstudy device to achieve PV isolation was considered an acute procedural failure. The prespecified performance goal was 90%.
e. Primary adverse events included major vascular access complication or bleeding, myocardial infarction, pericarditis, pulmonary oedema, stroke or cerebrovascular accident, transient ischemic attack, thromboembolism, heart block, vagal nerve injury or gastroparesis, cardiac tamponade or perforation (up to 30 days post-procedure), and permanent phrenic nerve paralysis as well as PV stenosis, atrioesophageal fistula, and death (up to 90 days post-procedure). The protocol-defined performance goal was 12%. The safety evaluation was also conducted in a subset of patients (n=31) undergoing cardiac CT/MRA imaging for PV narrowing, neurological assessment for cerebral lesion including silent cerebral lesion, and esophageal endoscopy for esophageal thermal injury in a prospective manner. The primary adverse events reported in SmartfIRE were 2 PV stenosis, 2 cardiac tamponade/perforation, 1 stroke, and 1 pericarditis; all resolved without clinical sequelae. The primary adverse event adjudication based on specific energy type (RF or PF) was not an option and would have helped to further understand the relationship between adverse events and energy.
f. CTI ablation was included.
g. The PF ablations with all applications <100% status were excluded and considered as invalid; the time spent on energy delivery was counted as ablation time, excluding the intervals between each delivery.
h. At baseline, 27/134 (20.1%) patients had hospitalizations related to CV events, compared with 16/134 (11.9%) patients during the 12 months after ablation. The use of Class I/III AADs reduced to 23.9% (32/134), resulting in a relative reduction of 60.4% compared to baseline (P<0.001 with McNemar test).
Abbreviations:
AAD, antiarrhythmic drug; AF, atrial fibrillation; AFEQT, Atrial Fibrillation Effect on Quality-of-Life; AFL, atrial flutter; AT, atrial tachycardia; CI, confidence interval; CT, computed tomography; CTI, cavotricuspid isthmus; CV, cardiovascular; DE STSF, Dual Energy THERMOCOOL SMARTTOUCH™ SF; ECG, electrocardiogram; ITD, intertag distance; LA, left atrial; MRA, magnetic resonance angiogram; PAE, primary adverse event; PAF, paroxysmal atrial fibrillation; PF, pulsed field; PFA, pulsed field ablation; PV, pulmonary vein; PVI, pulmonary vein isolation; RF, radiofrequency; SOC, standard of care; TTM, transtelephonic monitoring.
Reference:
- Duytschaever M, Račkauskas G, De Potter T, et al. Dual energy for pulmonary vein isolation using dual-energy focal ablation technology integrated with a three-dimensional mapping system: SmartfIRE 3-month results. Europace. 2024;26(5):euae088.
- De Potter T, Scherr D, Pürerfellner H, et al. Dual energy for pulmonary vein isolation using focal ablation technology integrated with a three-dimensional mapping system: SmartfIRE 12-month results. Europace. 2025;27(9):euaf174.
Additional DE STSF Platform publications:
- Di Biase L, Marazzato J, Zou F, et al. Point-by-point pulsed field ablation using a multimodality generator and a contact force-sensing ablation catheter: Comparison with radiofrequency ablation in a remapped chronic swine heart. Circulation: Arrhythmia and electrophysiology. 2023;16(12):663–671.
- Nakagawa H, Farshchi S, Maffre J, et al. Evaluation of ablation parameters to predict irreversible lesion size during pulsed field ablation. Circulation: Arrhythmia and electrophysiology. 2024;17(8):e012814.
- Verma A, Maffre J, Sharma T, et al. Effect of sequential, co-localized radiofrequency and pulsed field ablation on cardiac lesion size and histology. Circulation: Arrhythmia and Electrophysiology. 2025; 18(2):e013143.
- Kawamura I, Bhardwaj R, Govari A, et al. Coronary involvement with pulsed field ablation and radiofrequency ablation: preclinical insights. Circulation: Arrhythmia and Electrophysiology. 2025;18(1):e013161.
Disclosures:
The Dual Energy THERMOCOOL SMARTTOUCH™ SF Catheter and TRUPULSE™ Generator with Connection Interface Unit have received CE mark for use in the European Union but are currently investigational in the United States and have not been approved by the FDA.
Important information: Prior to use, refer to the instructions for use supplied with the device for indications, contraindications, side effects, warnings and precautions.
Always verify catheter tip location using common clinical practice for real-time verification (inspection of IC signals, direct imaging guidance such as fluoroscopy or ultrasound, etc.) and consult the CARTO™ 3 System User Guide regarding recommendations for fluoroscopy use.
Canpolat, U. et al (2020). State of Fluoroless Procedures in Cardiac Electrophysiology Practice. J Innov Cardiac Rhythm Management. 11(3), 4018–4029.
Sommer, P. et al (2018) Safety profile of near-zero fluoroscopy atrial fibrillation ablation with non-fluoroscopic catheter visualization: experience from 1000 consecutive procedures, EP Europace, Volume 20, Issue 12, Pages 1952–1958.
The THERMOCOOL SMARTTOUCH™ SF Catheter is indicated for the treatment of drug refractory recurrent symptomatic paroxysmal atrial fibrillation (AF) and for drug refractory recurrent symptomatic persistent AF (continuous AF > 7 days but < 1 year), refractory or intolerant to at least 1 Class I or III AAD, when used with the CARTO™ 3 System.
DO NOT use OCTARAY™ Mapping Catheter with TRUEref™ Technology in patients with prosthetic valves.
DO NOT use PENTARAY™ NAV ECO High Density Mapping Catheter or OCTARAY™ Mapping Catheter with TRUEref™ Technology in patients with prosthetic valves
This site is published by Johnson & Johnson and its affiliates. which is soley responsible for its contents. It is intended for visitors from the United States.
C_US_ELP_THER_403607.EN