Johnson & Johnson Institute
Laparoscopic sleeve gastrectomy
Operative steps
Potential complications include but are not limited to: Surgical bleeding, staple line leak, stricture, pseudo-stricture (narrowing at incisura, twisting of staple line during creation), DVT/pulmonary embolism, surgical site infection (deep or superficial).
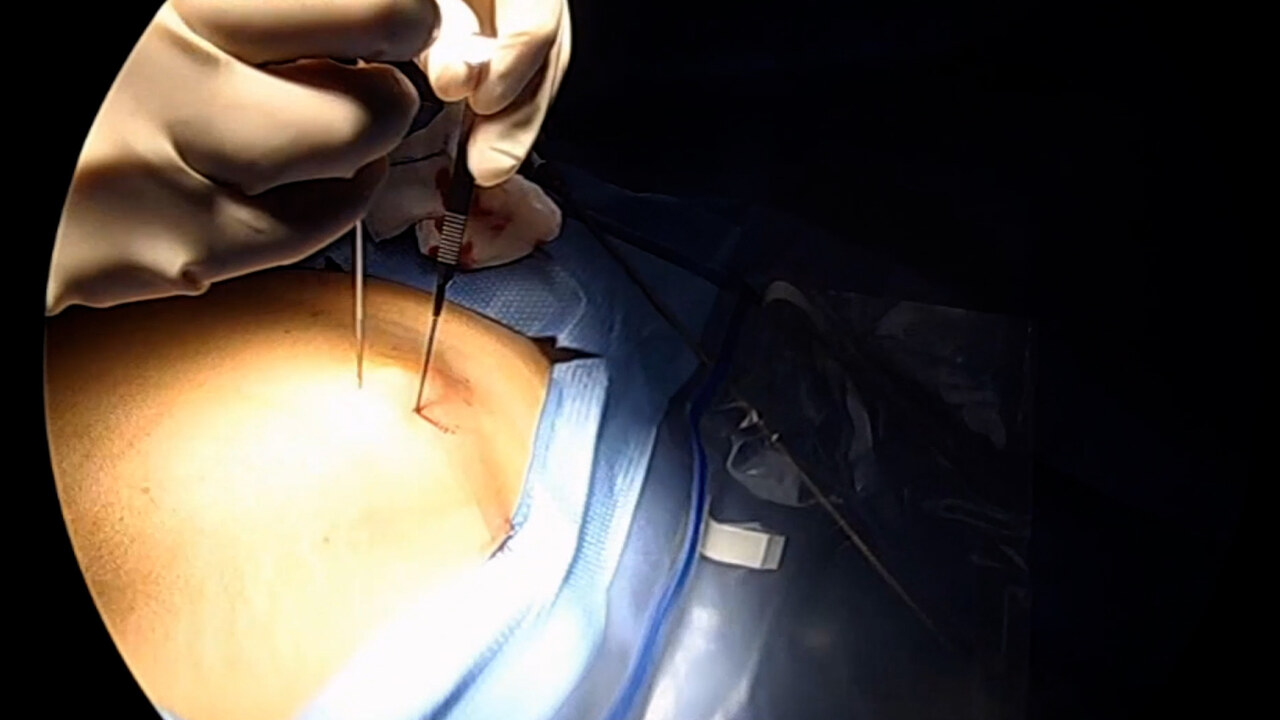
- Trocar sites are identified, and trocars inserted to gain access to the abdominal cavity and stomach. Generally, 4-5 trocars are required.
- Initial access to the abdomen is generally obtained by either:
- Veress needle technique
- Direct trocar view technique
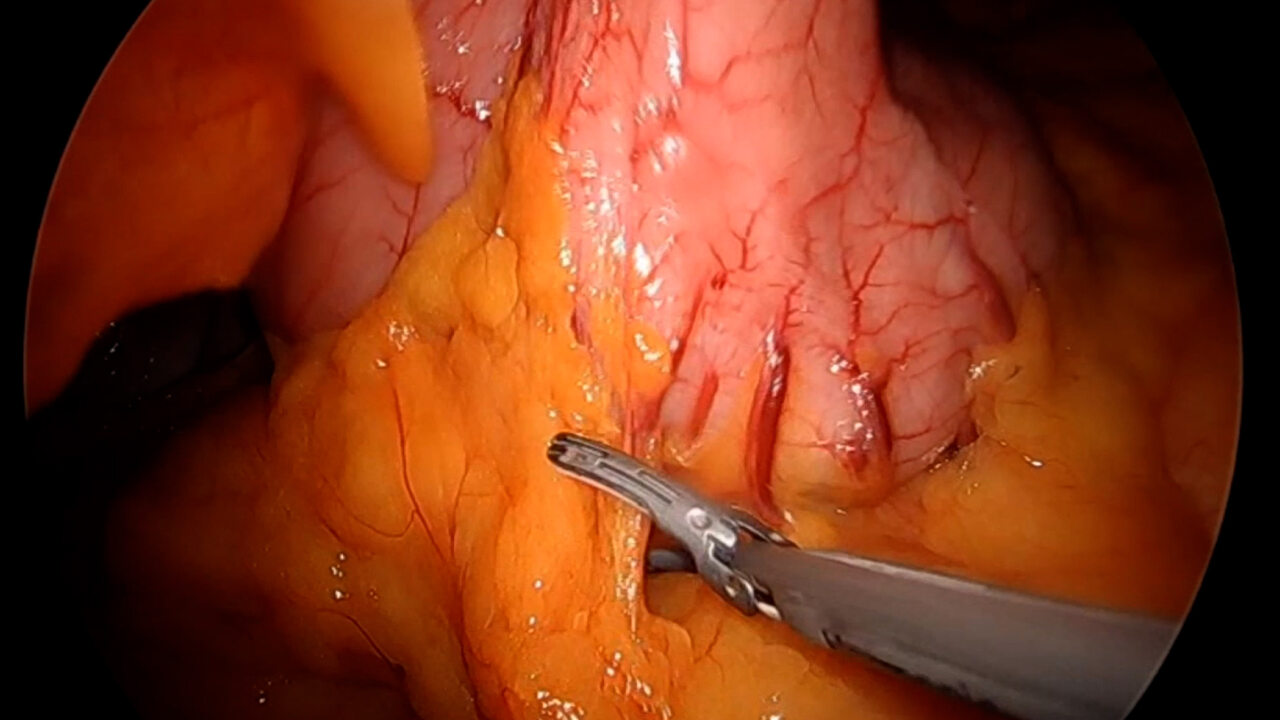
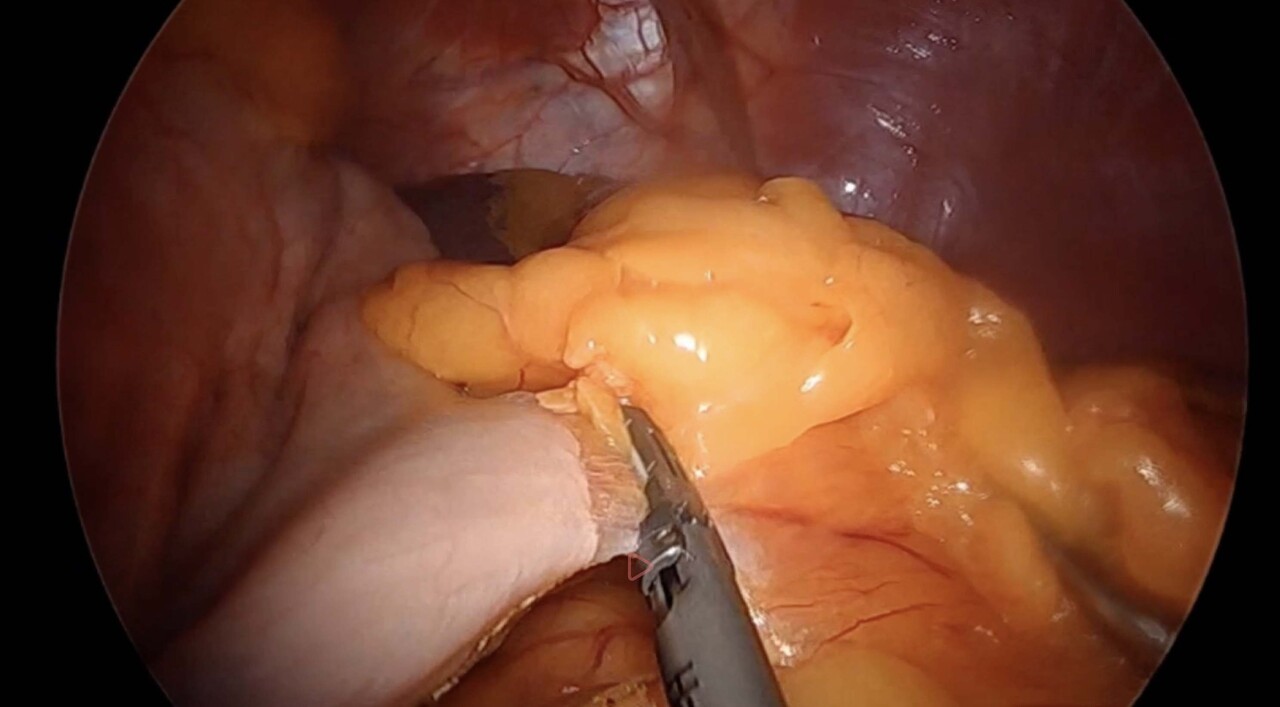
- Upon identifying the pylorus, the dissection begins at 4-6cm proximal to the pylorus.
- Attachments to the Greater curvature are mobilized with an energy device such as ENSEAL™ X1 Curved Jaw Tissue Sealer or HARMONIC™ 1100 Shears, including the short gastric vessels. The greater curve is mobilized completely to the diaphragm. If an ultrasonic energy device is used, completely encompassing the vessel that is being sealed, and allowing the device time to seal the vessels before lifting against the cutting blade, generally aids in achieving better hemostasis.
References
VISTASEAL™ Fibrin Sealant (Human) IMPORTANT SAFETY INFORMATION
INDICATION
VISTASEAL™, a fibrin sealant, is indicated as an adjunct to hemostasis for mild to moderate bleeding in patients undergoing surgery when control of bleeding by standard surgical techniques (such as suture, ligature, and cautery) is ineffective or impractical. VISTASEAL™ is effective in heparinized patients.
CONTRAINDICATIONS
Do not inject directly into the circulatory system.
Do not use for the treatment of severe or brisk arterial bleeding.
Do not use in patients with history of anaphylaxis or severe systemic reactions to human blood products.
Do not use VISTASEAL™ for spraying unless the minimum recommended distance from the applicator tip to the bleeding site can be achieved.
WARNINGS AND PRECAUTIONS
Thromboembolic events may occur if VISTASEAL™ is administered intravascularly.
Hypersensitivity reactions can occur.
May carry a risk of transmitting infectious agents, e.g., viruses, the variant Creutzfeldt-Jakob disease (vCJD) agent and, theoretically, the Creutzfeldt-Jakob disease (CJD) agent.
ADVERSE REACTIONS
The most common adverse reactions (reported in >1% of patients) were procedural pain, and nausea.
For complete indications, contraindications, warnings, precautions, and adverse reactions, please reference full package insert.
US_ETH_BIOS_110059.2
© Johnson & Johnson and its affiliates 2024
For complete indications, contraindications, warnings, precautions, and adverse reactions, please reference full package insert.
Christopher Joe Northup, MD prepared this procedure guide on behalf of Johnson & Johnson and its affiliates. The procedure guide reflects the opinions of the individual presenter, and the steps described may not encompass the complete steps of the procedure. Additionally, other surgeons may prefer different techniques, approaches, etc., as individual surgeon experience in his/her clinical practice, as well as patient needs, may dictate variation in procedure steps.
Before using any medical device, review all labeling, including without limitation; the Instructions For Use (IFU), and relevant package inserts with particular attention to the indications, contraindications, warnings and precautions, and steps for use of the device(s).
This presentation is not accredited for CE/CME.
Christopher Joe Northup, MD is compensated by and presenting on behalf of Johnson & Johnson and its affiliates and must present information in accordance with applicable regulatory requirements.
US_ETH_WOUN_117931