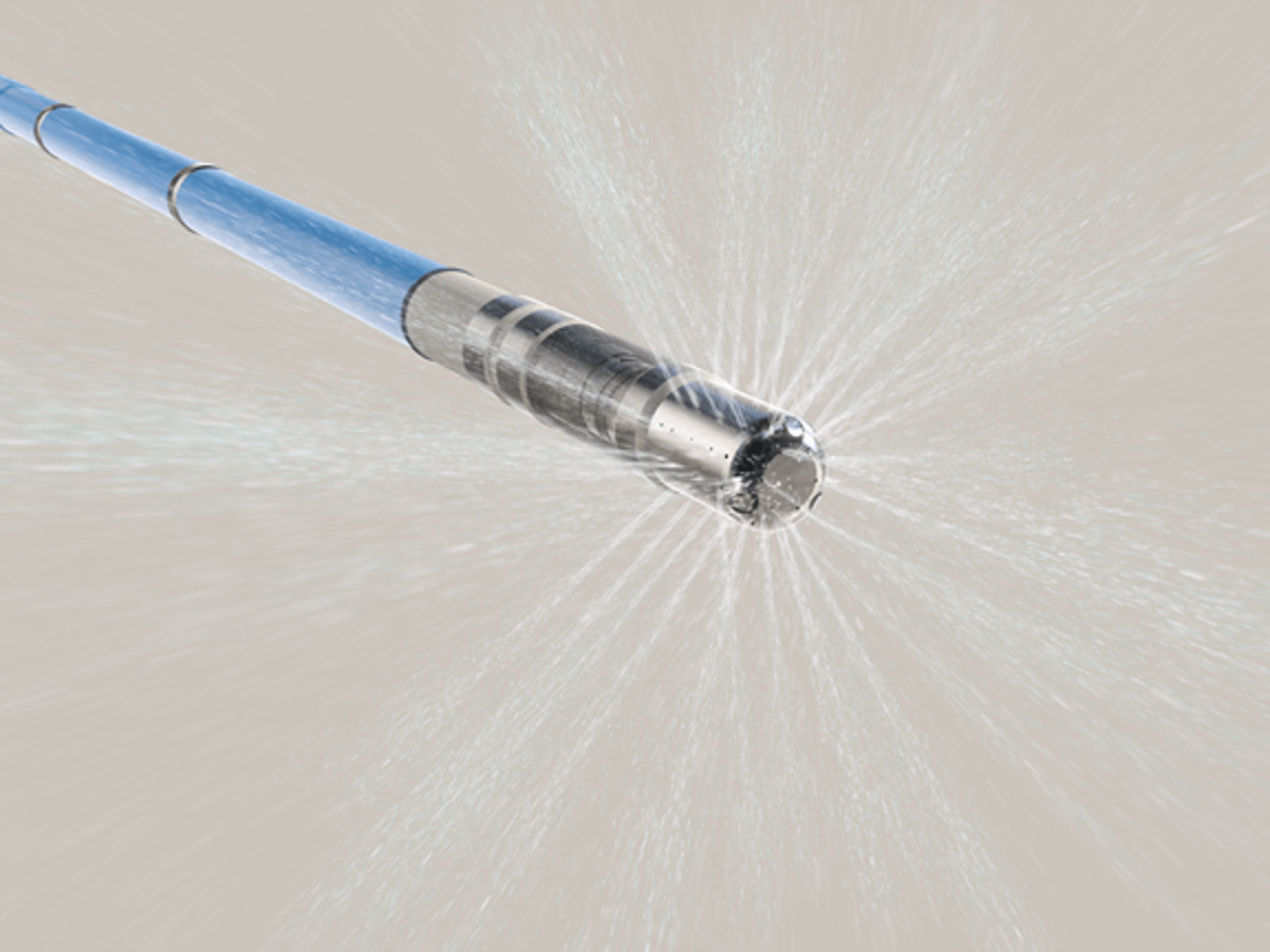
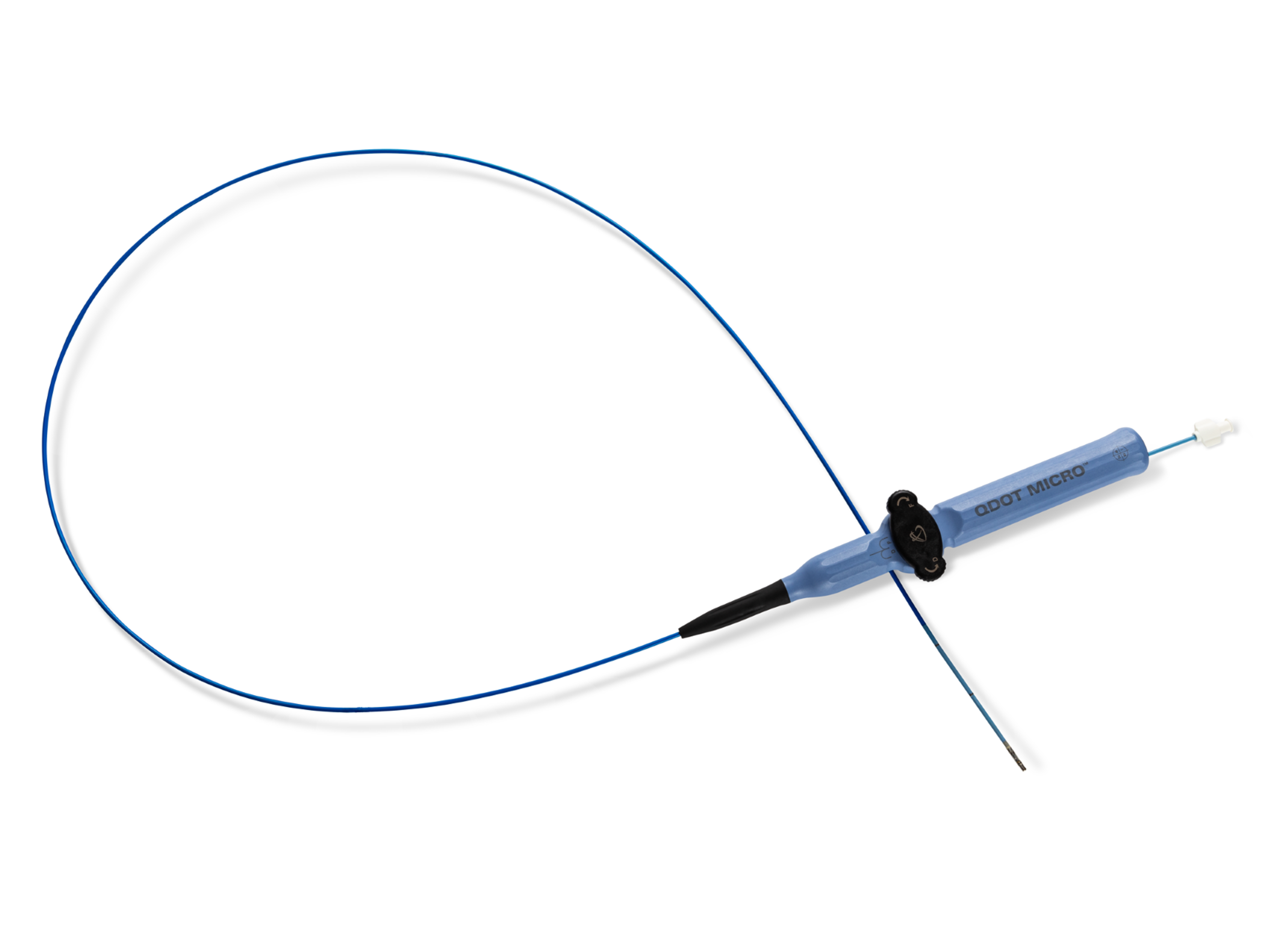
QDOT MICRO™ Catheter
QDOT MICRO™ Catheter has been designed to provide temperature control through automatic adjustment of power and fluid output based on real-time temperature measurement. Use of higher average RF power with QDOT MICRO™ Catheter is enabled by this optimized temperature control.2,4,5,6,8,13,14



Clinical evidence
Temperature-controlled ablation using the QDOT MICRO™ Catheter enhanced efficiency and efficacy without compromising safety.i,1,2,3, 6
89%
First pass isolation success rate4
Very high-power short duration (vHPSD) ablation was associated with 89% first-pass isolation success rate. Upon procedure completion, pulmonary vein isolation was achieved in 100% of patients. (n=46)
~60 min
Total procedure timeii,5
Based on real-world evidence examining ablations with the QDOT MICRO™ Catheter, a median procedure duration of ~60 minutes is achievable.
92%
Freedom from repeat ablation6
The effectiveness and freedom from a repeat ablation following a procedure with the QDOT MICRO™ Catheter was estimated to be 92.1% at 52 weeks.
Q-FFICIENCY prospective multi-center study (n=166): Kaplan-Meier estimate of freedom from repeat ablation.
↓84%
Shorter RF application timeviii,2,7,8,10
In the QDOT Q-FFICIENCY trial, QDOT MICRO™ Catheter had up to 84% shorter RF application time, when compared to conventional contact force catheters.
Indirect comparison of QDOT MICRO™ Catheter for RF application time: THERMOCOOL SMARTTOUCH™ SMART-SF (n=159; 49.5 min.) vs. QDOT-FAST Trial (n=52; 8.1 min.)
↓75%
Shorter mean fluoroscopy time6-12
RF ablation with the QDOT MICRO™ Catheter had up to 75% shorter mean fluoroscopy time compared to non-integrated PFA catheters.
Indirect comparison of QDOT MICRO™ Catheter to other ablation catheter clinical trials. PULSED AF Trial (PAF results; 26 min) vs. QDOT-FAST Trial (6.6 min)
88%
Patients reported an improved quality of life (QoL)11
88% of patients with an AF ablation using the QDOT MICRO™ Catheter, reported a clinically meaningful (>5 point) improvement in QoL from baseline.
Features & benefits
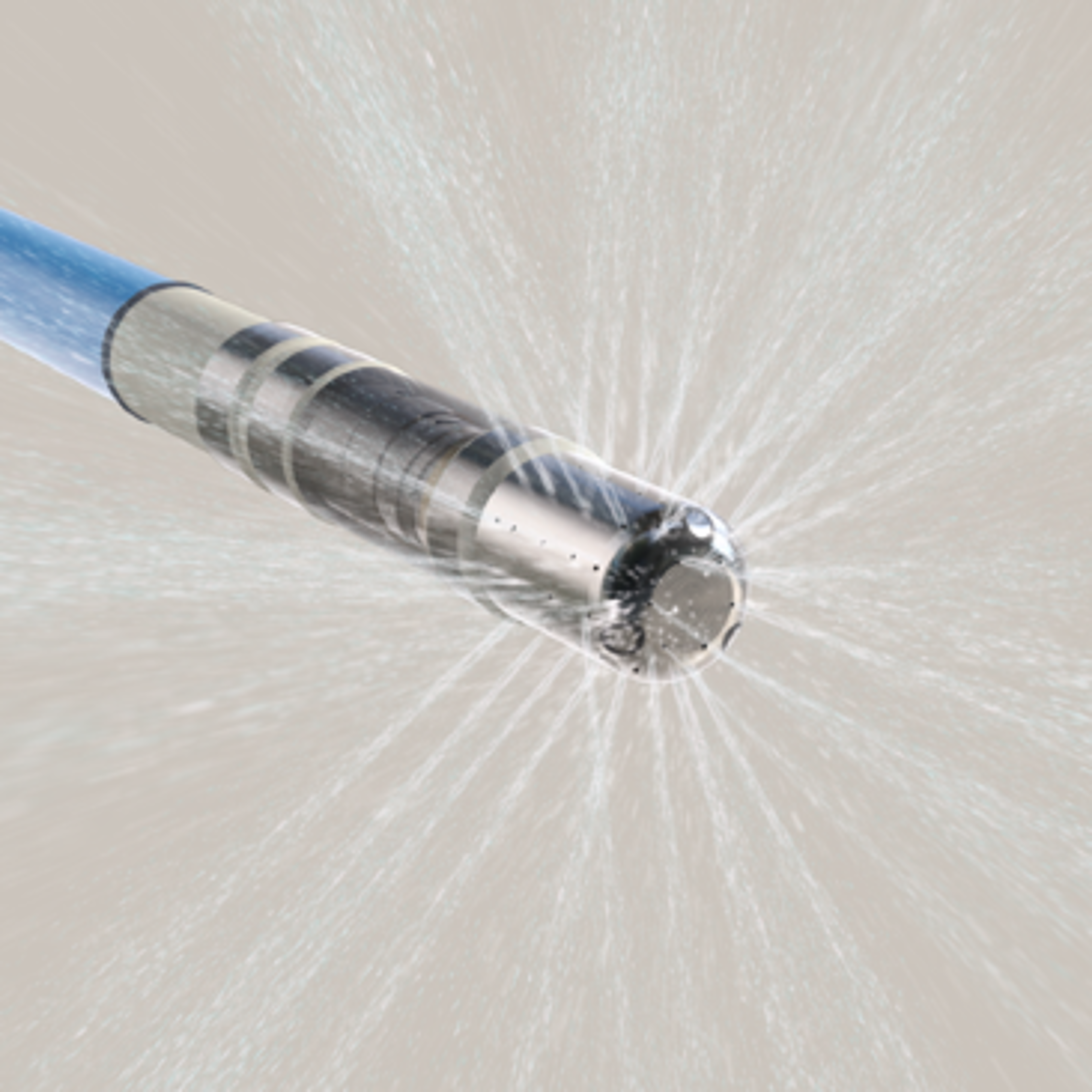
Optimized irrigationv, 7
Irrigation rate varies automatically for optimized power delivery, ensuring the tip is within the allowed target temperature range.7

Improved temperature monitoringvii, 7, 13
Temperature sensitivity that enables temperature control on an irrigated catheter with the addition of 6 thermocouples embedded into the tip.vi,12, 13

Higher signal resolutionv
QDOT MICRO™ Catheter includes 3 microelectrodes providing high resolution electrograms and discrete local signals.v

Advanced ablation
With QMODE+™ Module temperature control, the generator delivers the high RF energy at the set power for the set short duration or until the target temperature is reached.
An integrated system

nGEN™ Generator
.png?width=3840&quality=90&format=webp)
CARTO VIZIGO™ Bi-Directional Guiding Sheath

CARTO™ System Software

OCTARAY™ Mapping Catheter with TRUEref™ Technology

Dr. Jose Osorio
MD, FHRS
Supporting documentation
Related products

VARIPULSE™ Catheter
The VARIPULSE™ Platform’s full integration may reduce the need for multiple methods of catheter visualization used in one procedure, creating a streamlined workflow. Both clinical trial and real world evidence demonstrate the safety and value of VARIPULSE™ Platform.

THERMOCOOL™ Catheter
The catheter incorporates a thermocouple temperature sensor that is embedded in the 3.5 mm tip electrode. The high-torque shaft also allows the plane of the curved tip to be rotated to facilitate accurate positioning of the catheter tip at the desired site.

THERMOCOOL SMARTTOUCH™ SF Catheter
The porous tip of the catheter paired with contact force technology is designed to optimize efficiency. The THERMOCOOL SMARTTOUCH™ SF Catheter provides uniform cooling at half the flow rate of earlier generation irrigated catheters, easing the fluid management process.
References
i. Comparing data from nonrandomized, prospective, single-arm multicenter studies with similar designs: Q-FFICIENCY (n=166, Osorio et al 2022), NAVISTAR® THERMOCOOL IDE (n=139, Wilber et al, 2010), SMART-AF (n=160, Natale et al, 2014), and VISTAX (n=329, Duytschaever et al, 2020).
ii. Comparing data from nonrandomized, independent, prospective, single-arm multicenter studies with similar designs: Q-FFICIENCY (n=166, Osorio et al 2023), NAVISTAR THERMOCOOL IDE (n=139, Wilber et al, 2010), SMART-AF (n=160, Natale et al, 2014), and VISTAX (n=329, Duytschaever et al, 2020). The Q-FFICIENCY study safety performance goal was met; the posterior mean of the primary adverse event rate was 4.2%, with a 95% Bayesian credible interval of 1.7% to 7.7%, well below the 14% performance criterion. Based on the 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement (Calkins et al, 2017), the primary safety events observed in the Q-FFICIENCY study are in line with what is expected of catheter ablation studies for the treatment of atrial fibrillation.
iii. Based on Q-FFICIENCY, a prospective, nonrandomized, multicenter study with 166 evaluable participants ablated with the QDOT MICRO™ Catheter primarily with the QMODE+™ setting, alone or in combination with the QMODE™ setting.
iv. Data for conventional CF catheters is the average (122.6 min) of THERMOCOOL SMARTTOUCH SMART-AF (Natale et al, 2014; n=160, 121.5 min), THERMOCOOL SMARTTOUCH SMART-SF (Chinitz et al, 2018; n=159, 104.3 min), TactiCath TOCCATA (Reddy et al, 2012; n=34, 218.0 min), and TactiCath TOCCASTAR (Reddy et al, 2015; n=152, 46.5 min).
v. When compared to THERMOCOOL SMARTTOUCH™ Catheter and THERMOCOOL SMARTTOUCH™ SF Catheter
vi. Pre-clinical test data are not necessarily indicative of clinical performance.
vii. Based on a multicenter single arm study n=52. Improved temperature monitoring compared to traditional STSF catheter design with a single thermocouple.
vii i. Data for conventional CF catheters is the average (49.2 min) of THERMOCOOL SMARTTOUCH SMART-AF (Reddy et al, 2019, n=160, 60.6 min), THERMOCOOL SMARTTOUCH SMART-SF (Chinitz et al, 2018; n=159, 49.5 min), and TactiCath TOCCATA (Reddy et al, 2012, n=34, 37.6 min). QDOT Q-FFICIENCY (Osorio et al, 2022) reported a median RF application time, whereas all other studies reported mean RF application times
- Wilber DJ, Pappone C, Neuzil P, et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA. 2010;303:333-40.
- Natale A, Reddy VY, Monir G, Wilber DJ, Lindsay BD et al. (2014) Paroxysmal AF catheter ablation with a contact force sensing catheter: results of the prospective, multicenter SMART-AF trial. J Am Coll Cardiol 64 (7): 647-656.
- Duytschaever M, Vijgen J, De Potter T, et al. Standardized pulmonary vein isolation workflow to enclose veins with contiguous lesions: the multicentre VISTAX trial. Europace. 2020;22:1645-1652.
- Stabile G, Schillaci V, Strisciuglio T, et al. In vivo biophysical characterization of Very High Power, Short Duration, Temperature-Controlled Lesions. Pacing Clin Electrophysiol. 2021;44:1717
- Tilz RR et al. Very high-power short-duration temperature-controlled ablation versus conventional power-controlled ablation for pulmonary vein isolation: The fast and furious - AF study. IJC Heart & Vasculature. Volume 35, August 2021, 100847
- Osorio J, Hussein AA, Delaughter MC, et al. Very high-power short-duration, temperature-controlled radiofrequency ablation in paroxysmal atrial fibrillation: the prospective multicenter Q-FFICIENCY trial. JACC Clin Electrophysiol. Published online January 18, 2023. doi: 10.1016/j.jacep.2022.10.019.
- Reddy, VY et al. “Pulmonary Vein Isolation With Very High Power, Short Duration, Temperature-Controlled Lesions: The QDOT-FAST Trial.” JACC. Clinical electrophysiology vol. 5,7 (2019): 778-786. doi:10.1016/j.jacep.2019.04.009
- Chinitz, LA et al. “Safety and efficiency of porous-tip contact-force catheter for drug-refractory symptomatic paroxysmal atrial fibrillation ablation: results from the SMART SF trial.” Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology vol. 20,FI_3 (2018): f392-f400. doi:10.1093/europace/eux264
- Verma, A et al. “Pulsed Field Ablation for the Treatment of Atrial Fibrillation: PULSED AF Pivotal Trial.” Circulation vol. 147,19 (2023): 1422-1432. doi:10.1161/CIRCULATIONAHA.123.063988
- Reddy, VY et al. “Pulsed Field or Conventional Thermal Ablation for Paroxysmal Atrial Fibrillation.” The New England journal of medicine vol. 389,18 (2023): 1660-1671. doi:10.1056/NEJMoa2307291
- Hussein, AA et al. “Paroxysmal atrial fibrillation ablation with a novel temperature-controlled CF-sensing catheter: Q-FFICIENCY clinical and healthcare utilization benefits.” Journal of cardiovascular electrophysiology vol. 34,12 (2023): 2493-2503. doi:10.1111/jce.16093
- De Potter T, Grimaldi M, Jensen HK, et al. Temperature-Controlled Catheter Ablation for Paroxysmal Atrial Fibrillation: the QDOT-MICRO Workflow Study. J Atr Fibrillation. 2021;13(6):20200460.
- Leshem, E. et al (2018). High-Power and Short-Duration Ablation for Pulmonary Vein Isolation: Biophysical Characterization. JACC. Clinical electrophysiology, 4(4), 467–479.
- Calkins H, Hindricks G, Cappato R, Kim Y-H, Saad EB, et al. (2017) 2017 HRS_EHRA_ECAS_APHRS_SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. J Ep Europace 20 (1): e1-e160.
The VISITAG SURPOINT™ Module with EPU (VISITAG SURPOINT™ Module) is compatible with the QDOT MICRO™ Catheter. Equivalent Tag Index values do not represent equivalent RF lesion size. The recommended Tag Index target values for the THERMOCOOL SMARTTOUCH™ Catheter and THERMOCOOL SMARTTOUCH™ SF Catheter (i.e., 550 for anterior/roof/ridge segments and 380 for posterior/inferior segments of PV encircling lesions) should not be used to guide ablations with the QDOT MICRO™ catheter.
DO NOT use OCTARAY™ or OPTRELL™ Mapping Catheters with TRUEref™ Technology in patients with prosthetic valves.
The Johnson & Johnson and its affiliates QDOT MICRO™ Catheters and related accessory devices are indicated for catheter-based cardiac electrophysiological mapping (stimulating and recording) and, when used in conjunction with a compatible radiofrequency generator, for the treatment of:• Type I atrial flutter in patients age 18 or older.• Drug refractory recurrent symptomatic paroxysmal atrial fibrillation, when used with compatible three-dimensional electroanatomic mapping systems.The Johnson & Johnson and its affiliates QDOT MICRO™ Catheters provide real-time measurement of contact force between the catheter tip and heart wall, as well as location information when used with CARTO™ 3 Navigation System.
US_ELP_THER_339835.1